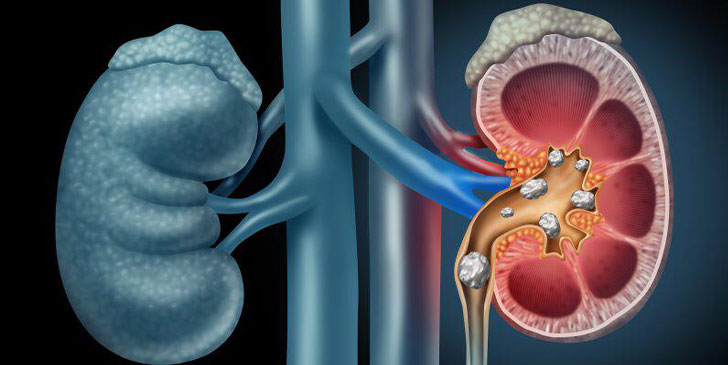
Renal calculi are formed when the urine is supersaturated with salt and minerals such as calcium oxalate, struvite (ammonium magnesium phosphate), uric acid and cystine. 60-80% of stones contain calcium.[2]They vary considerably in size from small 'gravel-like' stones to large staghorn calculi. The calculi may stay in the position in which they are formed, or migrate down the urinary tract, producing symptoms along the way. Studies suggest that the initial factor involved in the formation of a stone may be the presence of nanobacteria that form a calcium phosphate shell.
The other factor that leads to stone production is the formation of Randall's plaques. Calcium oxalate precipitates form in the basement membrane of the thin loops of Henle; these eventually accumulate in the subepithelial space of the renal papillae, leading to a Randall's plaque and eventually a calculus.
Bladder stones (calculi) account for around 5% of urinary tract stones and usually occur because of foreign bodies, obstruction or infection.[6]The most common cause of bladder stones is urinary stasis due to failure of emptying the bladder completely on urination, with the majority of cases occurring in men with bladder outflow obstruction.[7]Approximately 5% of bladder stones occur in women and are usually associated with foreign bodies such as sutures, synthetic tapes or meshes, and urinary stasis, so bladder stones should always be considered in women investigated for irritable bladder symptoms or recurrent urinary tract infections.[8]
Patients with indwelling Foley catheters are also at high risk for developing bladder stones and there appears to be a significant association between bladder stones and the formation of malignant bladder tumours in these patients.
Recurrence of renal stones is common and therefore patients who have had a renal stone should be advised to adapt and adopt several lifestyle measures which will help to prevent or delay recurrence:
• Increase fluid intake to maintain urine output at 2-3 litres per day.
• Reduce salt intake.
• Reduce the amount of meat and animal protein eaten.
• Reduce oxalate intake (foods rich in oxalate include chocolate, rhubarb, nuts) and urate-rich foods (eg, offal and certain fish).
• Drink regular cranberry juice: increases citrate excretion and reduces oxalate and phosphate excretion.
• Maintain calcium intake at normal levels (lowering intake increases excretion of calcium oxalate).
• Depending on the composition of the stone, medication to prevent further stone formation is sometimes given - eg, thiazide diuretics (for calcium stones), allopurinol (for uric acid stones) and potassium citrate (for oxalate stones).